

Volume 11, Issue 3 (Autumn 2025)
J Health Res Commun 2025, 11(3): 1-13 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
shahrokhi H, Ebrahimi E, Tarkhasi A. The Effect of Eight Weeks of Frankel’s Exercises on Balance, Reaction Time, Gait Parameters, and Quality of Life among Older Male Adults Attending Day Care Centers in Sabzevar. J Health Res Commun 2025; 11 (3) :1-13
URL: http://jhc.mazums.ac.ir/article-1-1178-en.html
URL: http://jhc.mazums.ac.ir/article-1-1178-en.html



Department of Sport Injury and Corrective Exercise, Faculty of Sport Sciences, Hakim Sabzevari University, Sabzevar, Iran.
Full-Text [PDF 6218 kb]
(550 Downloads)
| Abstract (HTML) (1437 Views)
References
Full-Text: (109 Views)
Introduction
With increasing life expectancy and the aging of the population in the world, including Iran, it is expected that by 2050, older people (aged 65 and older) will make up approximately 16% of the world’s population and 25% of Iran’s population. Age-related decline in sensorimotor function significantly increases the fall risk, compromising independence and quality of life in older adults. Physiological changes, including reduced muscle volume, strength, flexibility, agility, speed, and musculoskeletal capabilities, impaired balance and gait patterns, can lead to postural instability, falls, bone fractures, chronic pain, reduced mobility, and diminished movement independence.
Frankel’s exercises, which are based on proprioceptive neuromuscular facilitation (PNF), emphasize repetitive, slow, controlled movements in supine, sitting, and standing positions to enhance proprioception, coordination, and balance. Despite their potential for improving motor control, the simultaneous effects on static and dynamic balance, choice reaction time, gait speed, step length, and quality of life in older men over 75 years of age remain unclear. This group, due to mobility and environmental constraints, requires simple, low-cost interventions that do not require specialized equipment. Therefore, this study aimed to evaluate the impact of an eight-week Frankel exercise program on these variables in older men attending elderly day care centers in Sabzevar, Iran, providing evidence for its integration into fall prevention and rehabilitation programs for older adults.
Methods
This randomized controlled clinical trial was conducted on 40 inactive older men (<150 minutes of moderate-intensity activity per week) aged 75–85 years (mean age: 78.52±2.52 years) attending elderly day care centers in Sabzevar. From five centers, three were randomly selected, and participants were chosen proportionally based on the population of the centers and inclusion criteria: Ability to stand/walk 10 meters independently or with a cane, an MMSE score˃23 indicating no cognitive impairment, no use of medications affecting balance/central nervous system in the past four weeks, no uncontrolled diseases or severe musculoskeletal disorders. Exclusion criteria were: absence from ≥2 consecutive sessions or three sessions, injury, or unwillingness to continue participation. Sample size was calculated at 16 per group using G*Power (80% test power, α=0.05, effect size= 0.5), increased to 20, considering a 20% sample dropout. The block randomization method (block size of 4) was used to allocate groups. Participants and therapists were aware of allocation, but assessors and statisticians were blinded.
The intervention group (n=20) received 24 supervised sessions (3 sessions/week, 45–60 minutes): 10-minute warm-up, main protocol (supine/side-lying exercises such as knee/hip flexion, abduction/adduction, heel slides, bicycling, leg pressure; sitting exercises such as thigh lifts, sit-to-stand; standing exercises such as side/back/zigzag walking on heels/toes, 90-degree turns; 2 sets, 6–10 repetitions/5–10 seconds, progressive overload: +2 repetitions after 2 weeks, +1 set after 4 weeks), and 10-minute cool-down. The control group received usual care (with access to the post-study program). Pre-intervention and post-intervention (48 hours after the final session) assessments included static balance tests (Sharpened Romberg test with eyes-open/closed), dynamic balance (Timed up & go test), choice reaction time (Nelson’s modified test: 12.6 meters, 10 random right/left trials), gait speed/step length (8-meter walk, 3 trials), and quality of life (36- short form survey). Normality was confirmed by the Shapiro-Wilk test (P>0.05). The data were analyzed using a mixed ANOVA in SPSS software, version 27, with a significance level set at 0.05.
Results
Descriptive analysis confirmed group homogeneity in terms of age (control: 78.45±2.7 vs. intervention: 78.6 ±2.39 years, P=0.854), weight (68.6±5.74 vs. 66.25±6.43 kg, P=0.777), height (1.66±0.64 vs. 1.68±0.05 m, P=0.509), and BMI (24.02±2.18 vs. 23.41±1.96, P=0.356).
Mixed ANOVA results revealed significant time×group interaction effect (P<0.001) and main effects of time and group for all study outcomes. The intervention group demonstrated superior improvements (Table 1).
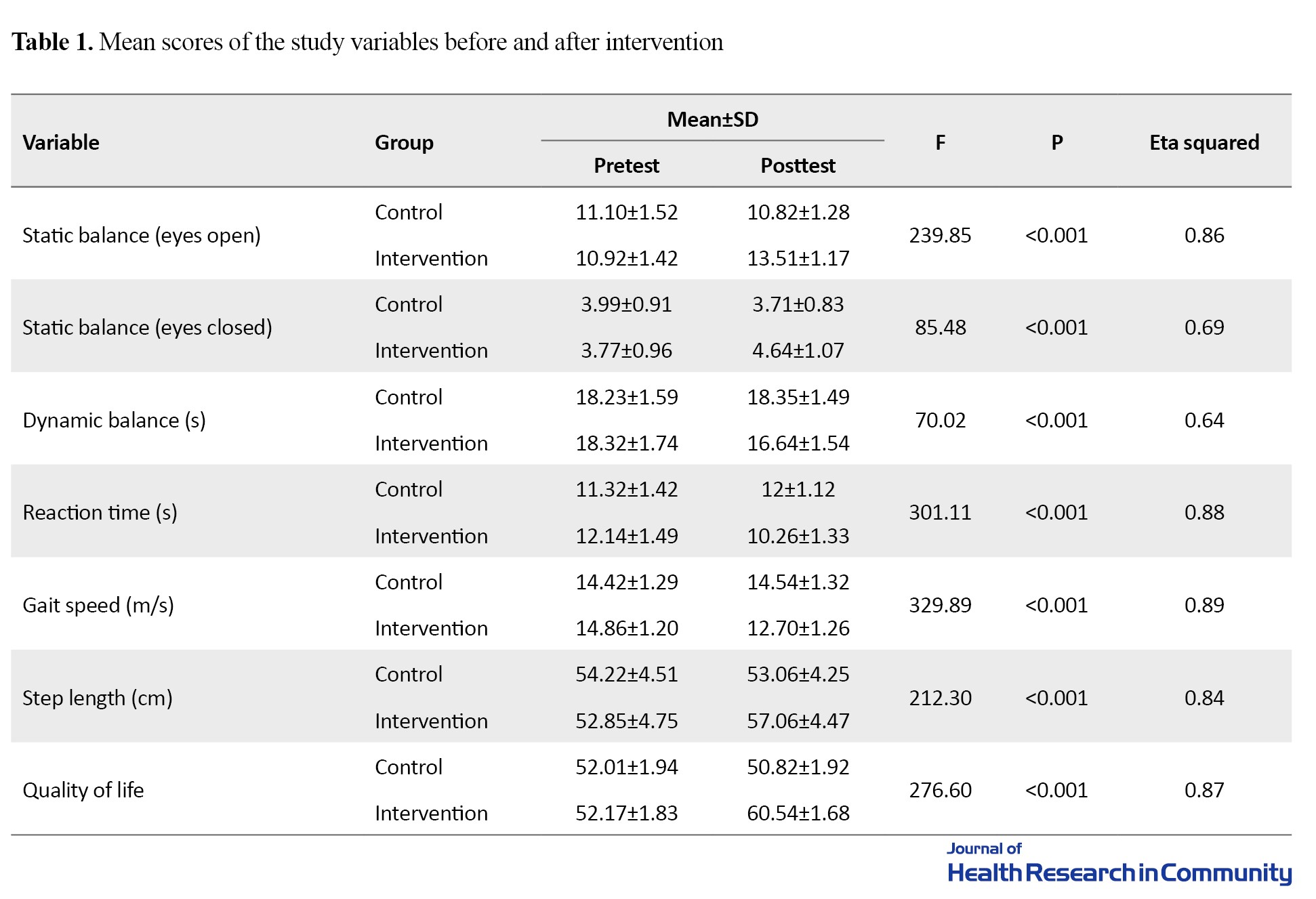
No adverse events were reported. Large effect sizes (η²>0.64) indicated strong clinical impact of the intervention.
Conclusion
An 8-week Frankel exercise program can significantly improve balance, reaction time, gait, and quality of life in older men aged >75. These findings support the integration of Frankel exercises into fall prevention and rehabilitation programs for older adults, particularly in institutional settings. Given their low cost, minimal equipment requirements, and absence of adverse effects, Frankel exercises offer a practical and promising strategy for enhancing functional independence in older men.
Ethical Considerations
Compliance with ethical guidelines
This study received ethical approval from the Ethics Committee of Hakim Sabzevari University (Code: IR.HSU.REC.1404.010). All participants provided written informed consent; they were informed of their rights, including the right to leave the study. No identifying information was used. The trial was registered by the Iranian Registry of Clinical Trials (ID: IRCT20220919055988N2).
Funding
This article was extracted from a research project at Hakim Sabzevari University. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Study design, supervision, editing & review: Hossein Shahrokhi; Exercise program implementation, initial draft preparation, statistical analysis, review: Ebrahim Ebrahimi; exercise program implementation, writing, data analysis: Abolfazl Tarkhasi; All authors read and approved the final version of the manuscript.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank all seniors, nurses, and managers of elderly day care centers in Sabzevar.
With increasing life expectancy and the aging of the population in the world, including Iran, it is expected that by 2050, older people (aged 65 and older) will make up approximately 16% of the world’s population and 25% of Iran’s population. Age-related decline in sensorimotor function significantly increases the fall risk, compromising independence and quality of life in older adults. Physiological changes, including reduced muscle volume, strength, flexibility, agility, speed, and musculoskeletal capabilities, impaired balance and gait patterns, can lead to postural instability, falls, bone fractures, chronic pain, reduced mobility, and diminished movement independence.
Frankel’s exercises, which are based on proprioceptive neuromuscular facilitation (PNF), emphasize repetitive, slow, controlled movements in supine, sitting, and standing positions to enhance proprioception, coordination, and balance. Despite their potential for improving motor control, the simultaneous effects on static and dynamic balance, choice reaction time, gait speed, step length, and quality of life in older men over 75 years of age remain unclear. This group, due to mobility and environmental constraints, requires simple, low-cost interventions that do not require specialized equipment. Therefore, this study aimed to evaluate the impact of an eight-week Frankel exercise program on these variables in older men attending elderly day care centers in Sabzevar, Iran, providing evidence for its integration into fall prevention and rehabilitation programs for older adults.
Methods
This randomized controlled clinical trial was conducted on 40 inactive older men (<150 minutes of moderate-intensity activity per week) aged 75–85 years (mean age: 78.52±2.52 years) attending elderly day care centers in Sabzevar. From five centers, three were randomly selected, and participants were chosen proportionally based on the population of the centers and inclusion criteria: Ability to stand/walk 10 meters independently or with a cane, an MMSE score˃23 indicating no cognitive impairment, no use of medications affecting balance/central nervous system in the past four weeks, no uncontrolled diseases or severe musculoskeletal disorders. Exclusion criteria were: absence from ≥2 consecutive sessions or three sessions, injury, or unwillingness to continue participation. Sample size was calculated at 16 per group using G*Power (80% test power, α=0.05, effect size= 0.5), increased to 20, considering a 20% sample dropout. The block randomization method (block size of 4) was used to allocate groups. Participants and therapists were aware of allocation, but assessors and statisticians were blinded.
The intervention group (n=20) received 24 supervised sessions (3 sessions/week, 45–60 minutes): 10-minute warm-up, main protocol (supine/side-lying exercises such as knee/hip flexion, abduction/adduction, heel slides, bicycling, leg pressure; sitting exercises such as thigh lifts, sit-to-stand; standing exercises such as side/back/zigzag walking on heels/toes, 90-degree turns; 2 sets, 6–10 repetitions/5–10 seconds, progressive overload: +2 repetitions after 2 weeks, +1 set after 4 weeks), and 10-minute cool-down. The control group received usual care (with access to the post-study program). Pre-intervention and post-intervention (48 hours after the final session) assessments included static balance tests (Sharpened Romberg test with eyes-open/closed), dynamic balance (Timed up & go test), choice reaction time (Nelson’s modified test: 12.6 meters, 10 random right/left trials), gait speed/step length (8-meter walk, 3 trials), and quality of life (36- short form survey). Normality was confirmed by the Shapiro-Wilk test (P>0.05). The data were analyzed using a mixed ANOVA in SPSS software, version 27, with a significance level set at 0.05.
Results
Descriptive analysis confirmed group homogeneity in terms of age (control: 78.45±2.7 vs. intervention: 78.6 ±2.39 years, P=0.854), weight (68.6±5.74 vs. 66.25±6.43 kg, P=0.777), height (1.66±0.64 vs. 1.68±0.05 m, P=0.509), and BMI (24.02±2.18 vs. 23.41±1.96, P=0.356).
Mixed ANOVA results revealed significant time×group interaction effect (P<0.001) and main effects of time and group for all study outcomes. The intervention group demonstrated superior improvements (Table 1).
No adverse events were reported. Large effect sizes (η²>0.64) indicated strong clinical impact of the intervention.
Conclusion
An 8-week Frankel exercise program can significantly improve balance, reaction time, gait, and quality of life in older men aged >75. These findings support the integration of Frankel exercises into fall prevention and rehabilitation programs for older adults, particularly in institutional settings. Given their low cost, minimal equipment requirements, and absence of adverse effects, Frankel exercises offer a practical and promising strategy for enhancing functional independence in older men.
Ethical Considerations
Compliance with ethical guidelines
This study received ethical approval from the Ethics Committee of Hakim Sabzevari University (Code: IR.HSU.REC.1404.010). All participants provided written informed consent; they were informed of their rights, including the right to leave the study. No identifying information was used. The trial was registered by the Iranian Registry of Clinical Trials (ID: IRCT20220919055988N2).
Funding
This article was extracted from a research project at Hakim Sabzevari University. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
Study design, supervision, editing & review: Hossein Shahrokhi; Exercise program implementation, initial draft preparation, statistical analysis, review: Ebrahim Ebrahimi; exercise program implementation, writing, data analysis: Abolfazl Tarkhasi; All authors read and approved the final version of the manuscript.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank all seniors, nurses, and managers of elderly day care centers in Sabzevar.
References
- Mohammadzadeh S. [The effects of multisensory balance training on balance performance and fall risk reduction in elderly: A semi-experimental study (Persian)]. J Healthy Ageing Exerc. 2025; 1(1):16-28. [DOI:10.18502/tbj.v23i3.16485]
- Farrokhnejad Z, Hosseini Abrishami L, Yazdan shenas A, Saeedeh Hosseini S. [The effect of eight weeks of selected vestibular exercises on functional balance, walking speed and quality of life of sedentary elderly men (Persian)]. J Tolooebehdasht. 2024; 23(3):92-106. [DOI:10.18502/tbj.v23i3.16485]
- Arghavani H, Zolaktaf V, Lenjannejadian S. Comparing the effects of anticipatory postural adjustments focused training and balance training on postural preparation, balance confidence and quality of life in elderly with history of a fall. Aging Clin Exp Res. 2020; 32(9):1757-65. [DOI:10.1007/s40520-019-01358-5] [PMID]
- Martínez-Amat A, Hita-Contreras F, Lomas-Vega R, Caballero-Martínez I, Alvarez PJ, Martínez-López E. Effects of 12-week proprioception training program on postural stability, gait, and balance in older adults: A controlled clinical trial. J Strength Cond Res. 2013; 27(8):2180-8. [DOI:10.1519/JSC.0b013e31827da35f] [PMID]
- Shohani M, Mohammadnejad S, Khorshidi A, Kiani SM. Effectiveness of aerobic exercise on dimensions of quality of life in elderly females. J Nurs Midwifery Sci. 2019; 6(3):112-7. [DOI:10.4103/JNMS.JNMS_9_19]
- Farsi A, Ashayeri H, Mohammadzadeh S. [The effect of six weeks balance training program on kinematic of walking in women elderly people (Persian)]. Iran J Ageing. 2015; 9(4):278-87. [Link]
- Zakaria NA, Kuwae Y, Tamura T, Minato K, Kanaya S. Quantitative analysis of fall risk using TUG test. Comput Methods Biomech Biomed Engin. 2015; 18(4):426-37. [DOI:10.1080/10255842.2013.805211] [PMID]
- Mohamed AA, El-Shamaa ET, Mohamed JAE-R. Assess the effect of exercises program on balance and prevention of recurrent falling among elderly people. Minia Sci Nurs J. 2019; 6(1):63-70. [DOI:10.21608/msnj.2022.136170.1024]
- Noruzi Z. The effect of four weeks of selected balance exercises on reducing the risk of falling inactive elderly women with balance defects. J Motor Behav Sci. 2020; 3(2):123-7. [Link]
- Ko EJ, Chun MH, Kim DY, Kang Y, Lee SJ, Yi JH, et al. Frenkel’s exercise on lower limb sensation and balance in subacute ischemic stroke patients with impaired proprioception. Neurol Asia. 2018; 23(3):217. [Link]
- Chundakal D, Kulkarni P, Chavan S, Prabhakar R. Effect of music therapy and frenkel exercise on reaction time in geriatric population-A comparative study. Indian J Physiother Occup Ther. 2021; 15(4):17. [DOI:10.37506/ijpot.v15i4.16491]
- Tarakci E, Tarakci D, Hajebrahimi F, Budak M. Supervised exercises versus telerehabilitation. Benefits for persons with multiple sclerosis. Acta Neurol Scand. 2021; 144(3):303-11. [DOI:10.1111/ane.13448] [PMID]
- Ghasemi E, Shayegannejad V, Ashtari F, Chitsaz A. [The effectiveness of Frenkel’s and Swiss ball exercises on improved balance and decreased depression in patients with multiple sclerosis: A comparative study (Persian)]. J Res Rehab Sci. 2011; 7(3):278-83. [DOI:10.22122/jrrs.v7i3.278]
- Mańko G, Pieniążek M, Tim S, Jekiełek M. The effect of frankel's stabilization exercises and stabilometric platform in the balance in elderly patients: A randomized clinical trial. Medicina. 2019; 55(9):583. [DOI:10.3390/medicina55090583] [PMID]
- World Health Organization (WHO). Working for health 2022-2030 action plan. Geneva: World Health Organization; 2022. [Link]
- Silsupadol P, Shumway-Cook A, Lugade V, van Donkelaar P, Chou LS, Mayr U, et al. Effects of single-task versus dual-task training on balance performance in older adults: A double-blind, randomized controlled trial. Arch Phys Med Rehabil. 2009; 90(3):381-7. [DOI:10.1016/j.apmr.2008.09.559] [PMID]
- Buchner DM, Cress ME, de Lateur BJ, Esselman PC, Margherita AJ, Price R, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol A Biol Sci Med Sci. 1997; 52(4):M218-24. [DOI:10.1093/gerona/52A.4.M218] [PMID]
- Moshref-Razavi S, Sohrabi M, Sotoodeh MS. [Effect of neurofeedback interactions and mental imagery on the elderly’s balance (Persian)]. Iran J Ageing. 2017; 12(3):288-99. [DOI:10.21859/sija.12.3.288]
- Corbin CB, Le Masurier GC. Fitness for life. Champaign: Human Kinetics; 2014. [Link]
- Hemayattalab R, Gaeini A. [Study of reflect power and action speed of 11-14 year student with nelsons test (Persian)]. Olympic. 2002; 22(3):49-56. [Link]
- Khezri A, Arab Ameri E, Hemayattalab R, Ebrahimi R. [The effect of sports and physical activity on elderly reaction time and response time (Persian)]. Iran J Ageing. 2014; 9(2):106-13. [Link]
- Ware JEJ, Sherbourne CD. The MOS 36-ltem Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med Care. 1992; 30(6):473-83. [DOI:10.1097/00005650-199206000-00002] [PMID]
- Ware JE Jr, Gandek B. Overview of the SF-36 health survey and the international quality of life assessment (IQOLA) project. J Clin Epidemiol. 1998; 51(11):903-12. [DOI:10.1016/S0895-4356(98)00081-X] [PMID]
- Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The short form health survey (SF-36): Translation and validation study of the Iranian version. Qual Life Res. 2005; 14(3):875-82. [DOI:10.1007/s11136-004-1014-5] [PMID]
- Moradi F, Parnian Y, Sakinepoor A, Norouzi Z, Mazidi M. Effect of frenkel’s training on gait, postural stability and balance in elderly women with kyphosis. J Health Care. 2021. [DOI:10.52547/jhc.23.2.121]
- Frankel R, Graber T. Realization of functional orthopedics using the frankel exercise device. In: Graber T, editor. Physiologic principles of functional appliances. St. Louis: CV Mosby. [Link]
- Langoni CDS, Resende TL, Barcellos AB, Cecchele B, da Rosa JN, Knob MS, et al. The effect of group exercises on balance, mobility, and depressive symptoms in older adults with mild cognitive impairment: A randomized controlled trial. Clin Rehabil. 2019; 33(3):439-49. [DOI:10.1177/0269215518815218] [PMID]
- Witte K, Emmermacher P, Pliske G. [Improvement of balance and general physical fitness in older adults by karate: A randomized controlled trial (German)]. Complement Med Res. 2017;24(6):390-393. [DOI:10.1159/000479151] [PMID]
- Ghaderiyan M, Ghasemi G, Lenjannejadian S, Sadeghi Demneh E. [The effect of turning training in comparison with balance training on balance performance, mobility, turning and fear of falling in older adults (Persian)]. Stud Sport Med. 2022; 14(32):43-76. [DOI:10.22089/smj.2022.12339.1583]
- Davranche K, Burle B, Audiffren M, Hasbroucq T. Physical exercise facilitates motor processes in simple reaction time performance: An electromyographic analysis. Neurosci Lett. 2006; 396(1):54-6. [DOI:10.1016/j.neulet.2005.11.008] [PMID]
- Waheed A, Azharuddin M, Ahmad I, Noohu MM. Whole-body vibration, in addition to balance exercise, shows positive effects for strength and functional ability in patients with diabetic peripheral neuropathy: A single-blind randomized controlled trial. J Diab. 2021; 12(4):456-63. [DOI:10.4103/jod.jod_47_21]
- Erdoğanoğlu Y, OKTAR BE, BODUR F. Effect of reaction time exercises on physical functionality and quality of life in geriatrics: A non-controlled study. Bezmialem Sci. 2024; 12(1):7-14. [DOI:10.14235/bas.galenos.2023.43660]
- Babaei Khorzoghi M. [The effectiveness of a six-week selective rotary exercises program on the spatial and temporal gait parameters in elderly men (Persian)]. Hayat. 2020; 26(3):251-65. [Link]
- Viswanathan A, Sudarsky L. Balance and gait problems in the elderly. Handb Clin Neurol. 2012; 103:623-34. [DOI:10.1016/B978-0-444-51892-7.00045-0] [PMID]
- Yalfani A, Sahab Gholifar M, Raeisi Z, Asgarpoor Kaji A. [Effect of virtual reality training on quality of life and risk of falling in older men with nonspecific low back pain (Persian)]. J Mod Med Inf Sci. 2023; 9(2):144-55. [DOI:10.32598/JMIS.9.2.4]
- Jones T, Moore T, Choo J. The impact of virtual reality on chronic pain. Plos One. 2016; 11(12):e0167523. [DOI:10.1371/journal.pone.0167523] [PMID]
- Ahmadi M, Noudehi M, Esmaeili M, Sadrollahi A. [Comparing the quality of life between active and non-active elderly women with an emphasis on physical activity (Persian)]. Iran J Ageing. 2017; 12(3):262-75. [DOI:10.21859/sija.12.3.262]
- Azizi M, Salehian M, Mazloom SR. [The effect of leisure time physical activity program on activities of daily living and hope in elderly men (Persian)]. J Gerontol. 2023; 8(6):82-95. [Link]
Type of Study: Research(Original) |
Subject:
Geriatric Medicine
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
